 Donate to ICIJ
Donate to ICIJ  Chelsea FC fined millions over secret payments under Abramovich ownership
Chelsea FC fined millions over secret payments under Abramovich ownership  Nearly half of powerful .50-caliber ammo seized by Mexican government came from US Army plant, defense minister says
Nearly half of powerful .50-caliber ammo seized by Mexican government came from US Army plant, defense minister says “Buying drugs isn’t about choice anymore – it’s about whatever’s available.” That’s how many drug users in northern Mexico describe how local illicit drug markets have transformed over the past decade.
Eugenia,* for instance, remembers when she began injecting heroin in Mexicali, a border city in the state of Baja California, around 25 years ago. Back then, getting the drug was a straightforward process. She bought in bulk from a trusted dealer — usually operating independently from Mexico’s large drug trafficking organizations — and could be almost certain that what she was buying was exactly what she wanted.
Today, Eugenia’s reality is starkly different. She now uses fentanyl, a synthetic opioid up to 50 times stronger than heroin. This wasn’t her choice. About 10 years ago, local distributors began covertly mixing fentanyl into heroin, introducing it without warning — and without users’ consent.
Several forces drove this shift. One was tied to broader dynamics in drug trafficking. Mexican criminal networks supplying the massive US opioid market found that fentanyl, at the time imported largely from China, had begun replacing heroin. As prices plunged and production slowed, many producers and traffickers turned to synthetic drugs, including fentanyl, which offered significant economic advantages. Unlike plant-based drugs, fentanyl could be easily mixed with other substances, trafficked in much smaller quantities, and required far less investment to produce.
The other driver came from within the criminal underworld itself. Over the past two decades, Mexico’s major drug trafficking organizations have undergone a prolonged fragmentation, splintering into smaller, more localized, and increasingly predatory factions. In Mexicali, for instance, the Rusos — once an armed wing of the Sinaloa Cartel — entrenched themselves in the city and surrounding areas to control a key border crossing. Over time, they shifted their focus toward dominating local criminal markets, with street-level drug peddling becoming one of their primary targets.
Independent dealers, like the ones Eugenia used to buy from, were pushed out or forced to fall in line. The Rusos imposed a strict system to ensure that only their authorized sellers could profit. Doses were standardized, packaging marked with authorization seals, and sales were tightly controlled — dictating exactly what could be sold, where, and by whom.
SEE ALSO: 5 Models of Criminal Control Over Fentanyl Markets in Northern Mexico
When fentanyl was introduced, the impact on the streets was devastating. Unaware that it had entered circulation, many users suffered overdoses and deaths that the Mexican government has yet to fully document. The drug also brought new health consequences: harsher withdrawal symptoms, heightened anxiety, intense physical pain, and severe skin lesions. But users had little choice. The Rusos controlled supply, and finding “pure” heroin became nearly impossible.
“I don’t like fentanyl, but it’s not like I can ask them to just sell me chiva [heroin],” Eugenia said. “Now, you can only buy what they give you.”
Her experience echoes that of dozens of users interviewed by InSight Crime over the past two years across the border states of Baja California, Sonora, and Chihuahua, where local drug markets have undergone similar transformations.
As international drug policy increasingly moves toward public health strategies, the experiences in northern Mexico suggest that criminal control over local markets, and the decisions criminal actors make about supply, can severely challenge these efforts.
Below, we examine four ways in which these dynamics have played out on the ground.
New Adulterants and Drug Mixing
By late 2023, many fentanyl users in Mexicali and Tijuana — another border city in Baja California heavily affected by fentanyl — had either developed a tolerance to the drug or learned safer ways to consume it, largely due to the efforts of local harm reduction organizations. For a time, this helped stabilize the number of overdose deaths.
Then, the situation changed.
Users suddenly began overdosing more frequently and more severely. Even after receiving naloxone, the opioid overdose antidote, some remained sedated for hours. Others developed severe open wounds on their skin, sometimes leading to necrosis, unlike anything they had seen before. Reports of heightened anxiety and panic attacks also became increasingly common.
Alarmed, local community-based organizations began conducting tests and discovered that xylazine, a veterinary sedative not approved for human use, had quietly entered the fentanyl supply.
The source traced back to fentanyl production in the state of Sinaloa. Facing a temporary shortage of key chemical precursors, InSight Crime found that many producers had turned to xylazine and other veterinary tranquilizers, like zoletil, to stretch the volume of their product and increase profits. These batches were later mixed with unadulterated fentanyl shipments before reaching retail markets.
By the time the drugs hit the streets, it was impossible to know which doses contained xylazine. Neither dealers nor users could tell — until they consumed it.
“For the first time, I really didn’t know what I was putting in my body,” Eugenia said.
In response, community-based organizations began urging users to bring their paraphernalia and drug packaging for testing with strips that detect xylazine, allowing them to know in advance whether their dose contained it. The wave passed quickly, underscoring just how volatile synthetic drug markets can be. By April 2024, when public health authorities finally issued an official alert, xylazine had virtually disappeared from Tijuana and Mexicali’s streets.
SEE ALSO: How Fentanyl Was Introduced in Mexico’s Local Drug Markets
Now, another concern has surfaced for treatment providers, outreach workers, and emergency personnel across the border. Polydrug contamination, particularly involving fentanyl and stimulant drugs, is pushing overdose risks into populations beyond opioid users.
In May 2025, five young people died in Ciudad Juárez, Chihuahua, after consuming what they believed was cocaine. Toxicology tests later revealed they had consumed cocaine mixed with traces of fentanyl. The cases were scattered across the city, and no similar overdoses were recorded in the following months, leading authorities to conclude the deaths were tied to a single contaminated shipment, according to InSight Crime interviews. Still, emergency personnel worried that another tainted shipment could arrive at any time, with no way to predict when.

Elsewhere, in Tijuana, the director of a network of treatment centers, speaking on condition of anonymity, said that in June 2025 he began administering fentanyl-specific urine and blood tests to incoming patients. Among more than 400 patients his organization treats across the city, roughly 70 percent tested positive for fentanyl, yet only about 10 percent reported knowingly using it. The rest said they had consumed only methamphetamine.
This has complicated treatment protocols. The director noted that detox periods have become harder to manage. For example, methamphetamine users typically sleep for long stretches during withdrawal, but recently many experienced prolonged insomnia — a symptom more commonly associated with opioid withdrawal — followed by extreme hypersomnia, requiring constant adjustments to their medication.
“Even though we’ve managed to stabilize the fentanyl crisis, once new substances get mixed in, we’re back facing new challenges,” said Alfonso Chávez, who runs the harm reduction program at Prevencasa, a nonprofit based in Tijuana.
Altering Drug Potency
For many fentanyl users on the border, consumption has less to do with recreational effects and more to do with avoiding “la malilla,” the painful withdrawal symptoms the drug causes. But in early 2025, users in downtown Mexicali began noticing that the doses they bought at their usual local selling points were no longer strong enough to stave off withdrawal.
Eugenia, for example, who typically used two to three times a day, found herself nearly doubling her intake to achieve the desired effect.
Facing the same situation, many users began desperately searching for new points of sale, hoping to find stronger doses. Word spread quickly, and many moved through the city in groups. But each time they located a reliable source, the potency dropped again after only a few weeks, Eugenia and other users told InSight Crime. Within a couple of months, many were pushed to the city’s outskirts, the only place where stronger doses were still available.
The reasons behind this shift remain uncertain. Some sources suggested the reduction in purity was an order “from above”: a decision by the Rusos, possibly intended to push users out of the city center, which also serves as a popular tourist area and a hub for other criminal markets. Others believed it reflected the Rusos’ inconsistent fentanyl supply from Sinaloa, where criminal factions continue to engage in a bloody war, while other actors on the city’s outskirts reportedly still had access.
Whatever the intent, the change in potency had serious consequences for drug users.
SEE ALSO: Do Changes in Mexico’s Fentanyl Production Explain a Drop in US Overdoses?
First, users forced to the city’s outskirts searching for stronger doses faced a heightened risk of violence from criminal groups or harassment by police. The Rusos’ tight control over the drug market means that buying from actors outside their network can be deadly. Moreover, every user interviewed by InSight Crime cited detention or extortion by police while moving around the city as one of their greatest concerns.
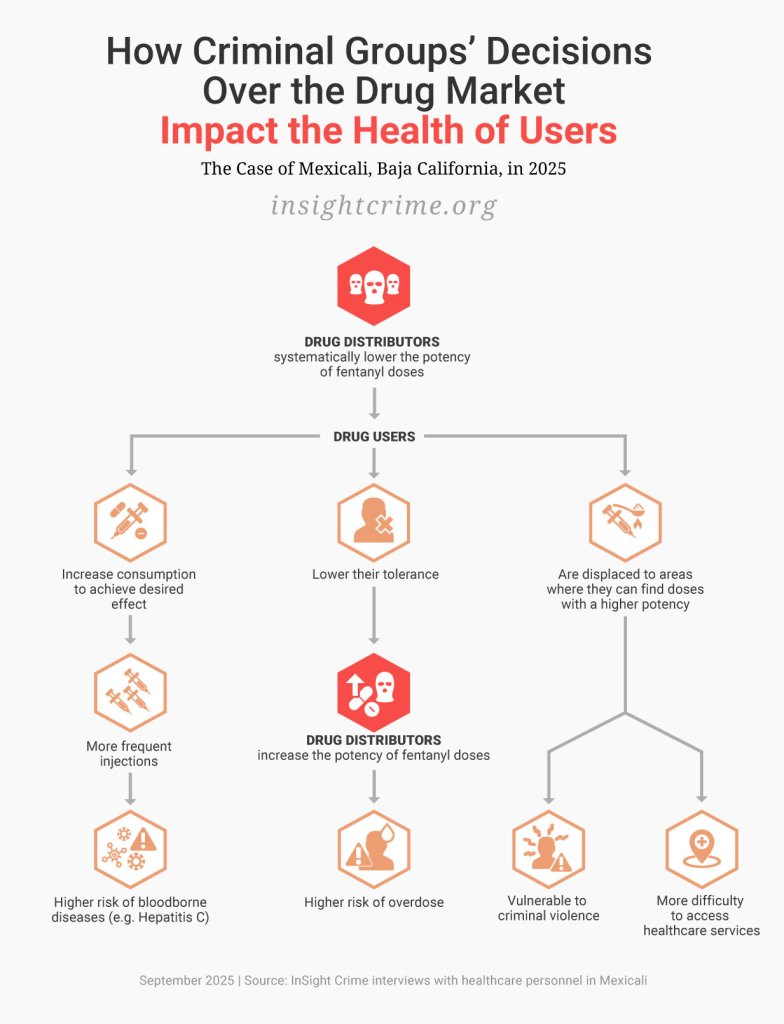
The second impact was reduced access to healthcare and harm reduction services. Once users located a dealer selling doses potent enough to ease withdrawal, they tended to stay nearby, as they needed to buy multiple times per day. This meant being far from downtown Mexicali, where most healthcare services are concentrated, including medical treatment, syringe exchange programs, and access to naloxone. Harm reduction workers told InSight Crime that attendance at these services declined during this period of scarcity.
Third, for those unable to find stronger doses, the only way to ease withdrawal symptoms was to increase consumption, as in Eugenia’s case. This meant more injections per day, which heightened the risk of contracting blood-borne diseases when syringes were shared, as well as other injection-related infections. While updated public statistics are unavailable, a municipal health worker in Mexicali, speaking on background because she was not authorized to speak publicly, told InSight Crime that she has observed an apparent rise in hepatitis C cases among users since the start of the year, coinciding with these shifts.

Finally, inconsistent potency also disrupts users’ tolerance. As people regularly consume weaker doses, their tolerance to fentanyl gradually decreases. As a result, if they unexpectedly consume a stronger batch, their risk of overdose rises sharply.
Local harm reduction workers told InSight Crime that this is exactly what happened. Around August 2025, the potency of downtown drugs increased again after several months, triggering a spike in overdoses.
“For us, this is still a crisis. The lack of consistency in fentanyl concentrations continues to drive overdose peaks,” said Lourdes Angulo, director of Verter A.C., a local harm reduction organization.
Imposing Restrictions on the Market
In some cities, criminal groups have taken a far more restrictive approach to fentanyl than in Mexicali and Tijuana.
Take Nogales, a border city in the state of Sonora with another long-standing population of heroin users. For years, access to heroin in Nogales has been controlled by factions of the Sinaloa Cartel and the Salazar, a local family clan that has consolidated control over some trafficking routes in Sonora. In many ways, both groups have prioritized maintaining secure cross-border operations over fostering a local drug market.
As a result, heroin availability has fluctuated, with brief periods of access often followed by prohibitions that create scarcity. Distribution has largely been handled by independent “clandestine” actors connected to the international drug trade but operating outside the control of dominant criminal groups. This has made the local market dangerous for users.
In this context, fentanyl pills — already trafficked in large quantities across the Nogales border — entered the local market in 2016. These were introduced by clandestine actors as an alternative for heroin users during a period of scarcity. While the pills eased withdrawal symptoms, users told InSight Crime that they also caused overdose spikes they had never experienced with heroin. And they produced a more severe addiction. Users could no longer go days without consuming, or they experienced intense pain, anxiety, panic attacks, and insomnia. The need to find the next pill quickly became urgent and all-consuming.
Criminal prohibitions, however, made this search extremely risky. Several users interviewed by InSight Crime said they had been tortured for seeking fentanyl and knew people who had been killed or disappeared by the local criminal groups for selling or consuming it. Yet with no legal alternatives — methadone treatments have been unavailable in Nogales since 2020 — and heroin no longer providing relief, users took the risk.
“Once you consume fentanyl, heroin is like water. It does nothing to relieve withdrawal. That’s why you feel a desperate urgency to find the pills,” a fentanyl user in Nogales told InSight Crime.

The city’s violent and highly controlled environment has also stifled public health interventions to attend to these users. A municipal health worker, speaking anonymously for security reasons, said that in 2016 his team stopped visiting opioid consumption sites to offer services such as syringe exchanges, bloodborne disease testing, and medical care due to constant surveillance by criminal groups.
“Criminal groups prohibited opioid consumption in the city, so they threatened us whenever we went to these places. For security reasons, we were officially instructed to stop doing field interventions,” he said.
Even though services remained available at their offices, fentanyl users rarely sought them out. Moving through the city carries the risk of detention by criminal groups or police, and being caught with “prohibited” drugs, such as fentanyl pills, can be life-threatening. Many users are also afraid to admit they consume fentanyl, fearing they could be handed over to criminal groups.
With civil society organizations similarly constrained, fentanyl users’ only remaining option is abstinence-based treatment. These programs operate in private, often unregulated centers that frequently lack medications to ease withdrawal and are ill-equipped to manage fentanyl dependencies specifically. For many users, these centers function less as treatment options and more as places to hide when the streets become too dangerous.
“I felt like it was either the malilla [withdrawal symptoms] or the mafia who was going to kill me. That’s why I’m here,” a fentanyl user told InSight Crime at one of Nogales’ treatment centers.
In other cities, criminal groups have imposed different restrictions that, while less severe, still have serious health consequences. In the Sonoran capital of Hermosillo, for example, as well as in Mexicali, criminal groups have limited the sale of smoking pipes to authorized vendors. Smoking is a method of consumption that, while not without risks, has been associated with lower overdose rates and avoids injection-related infections. In Tijuana, the harm reduction organization Prevencasa has encouraged fentanyl users to make the switch and, at least anecdotally, has observed promising results.
However, in Hermosillo and Mexicali, criminal restrictions prevent civil society organizations and health authorities from distributing pipes as safer alternatives. As a result, many users continue injecting rather than risk running afoul of criminal actors.
Invisible Borders
In cities where multiple criminal groups control the drug market, these groups often establish strict territorial boundaries and dictate where and what users can buy or consume.
The border city of Ciudad Juárez provides a clear example. Street-level drug sales are controlled by criminal organizations and gangs that have effectively divided the city into micro-territories. These invisible borders are largely defined by which substances are permitted in each area.
Factions linked to the Juárez Cartel — including La Línea, La Empresa, and Barrio Azteca — control the central and northern parts of the city. In their territory, heroin, cocaine, and marijuana are permitted, but methamphetamine sales are strictly prohibited. By contrast, groups aligned with the Sinaloa Cartel — such as the Mexicles and Artistas Asesinos — dominate southern and peripheral neighborhoods, where methamphetamine, cocaine, and marijuana are allowed, but heroin is banned. In both areas, fentanyl use and distribution remain tightly restricted.
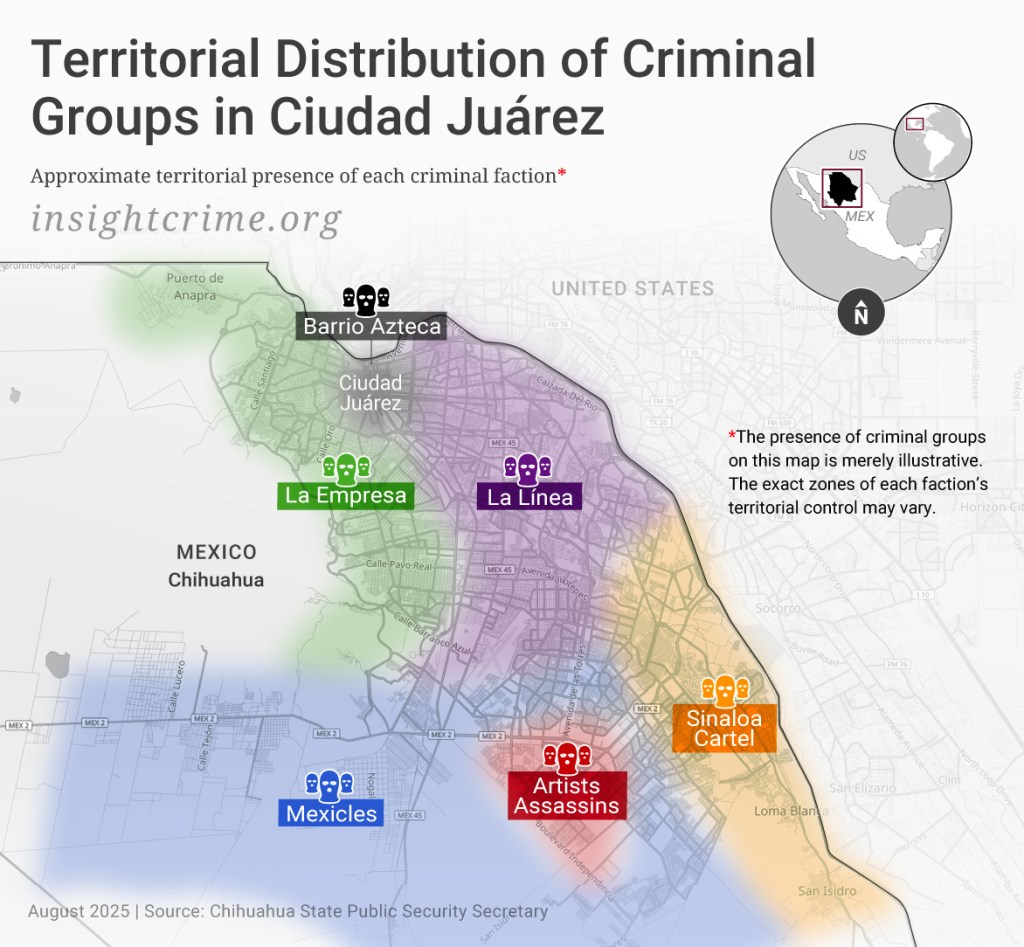
These rules are strictly enforced. Entering a neighborhood to buy or sell a “prohibited” drug can put both users and dealers at grave risk. Regional prosecutor Carlos Salas told InSight Crime that roughly 85% of homicides in Juárez are linked to the local drug trade, including violence stemming from the enforcement of these territorial boundaries.
But beyond fueling violence, these divisions also create major public health barriers. According to Lizeth Gutiérrez, regional head of the State Commission on Addiction (Comisión Estatal de Atención a las Adicciones — CEAADIC), about seven in 10 drug users in Juárez consume more than one substance. It is common to combine heroin with benzodiazepines or crack cocaine, and since methamphetamine began circulating widely in the late 2010s, some users also mix heroin and methamphetamine to balance or intensify the effects.
These patterns force many users to violate criminal rules and cross territorial boundaries to access the substances they want. Several users interviewed by InSight Crime said they consume alone and in hiding to avoid detection by criminal groups, which increases the risk of a fatal overdose, as no one is nearby to intervene. Fentanyl users face an even greater danger, since the drug is prohibited throughout the city.
Seeking treatment or medical services is equally risky. A local health official, speaking on condition of anonymity because they were not authorized to comment publicly, explained that many methamphetamine-injecting users avoid syringe exchange programs, blood-borne disease testing sites, and methadone substitution clinics, if they also use heroin, because most of these services are located in the city center, where methamphetamine use is restricted.
“Especially if, for some reason, they are associated with a rival gang, going into the wrong zone can get them killed,” the official said.
Even treatment centers must adapt to these restrictions. Another health worker, also speaking anonymously because they were not authorized to comment publicly, explained that referrals must follow the criminal boundaries: Heroin users tend not to be sent to clinics in areas where only methamphetamine is allowed, and methamphetamine users avoid facilities located in heroin-dominated zones.
For polydrug users, the situation is even more complex.
“For safety reasons, many do not disclose their use of methamphetamine or fentanyl when seeking treatment in certain areas,” the health worker said. “This makes it much harder to provide the appropriate care.”
*The name of the source has been changed for security reasons.
Angélica Ospina, Cecilia Farfán, Bianca Acuña, Steven Dudley, and Mike LaSusa contributed to this report.





