 Merck takes Austria’s Keytruda price transparency battle to top court as journalists fight for information
Merck takes Austria’s Keytruda price transparency battle to top court as journalists fight for information  China Deepens Economic Integration with Central Asia
China Deepens Economic Integration with Central Asia  Malaysia’s Anwar Faces Royal Upheaval
Malaysia’s Anwar Faces Royal Upheaval By Jenny Kitzinger, 10th July 2026
Editorial Note: This is the fifth ‘commentary’ blog post we have published in the wake of the Supreme Court decision, handed down in June 2026, changing more than a decade of law and practice on ‘deprivation of liberty’ (see Endnote for more information).
Since 2014, with the Supreme Court decision in Cheshire West, my profoundly brain-injured sister, Polly Kitzinger, has been “deprived of her liberty” in a series of neuro-rehabilitation centres and care homes.
Since 2nd June 2026, when the AGNI judgment[1] was handed down by the Supreme Court, effectively reversing Cheshire West, she is probably no longer deprived of her liberty, as a matter of law (though this hasn’t yet been confirmed), and it’s likely that she will soon cease to have access to the associated Deprivation of Liberty Safeguards [DoLS].
Nothing actually changed in the nature of Polly’s care or confinement on 2nd June 2026, except for the way the law now defines it.
The AGNI judgment says that a person is not deprived of her liberty if she is confined “because her condition was such as to require this by way of care” or the person is “wholly incapable of leaving both because of physical inability and because she was unable to form any desire or intention to leave” (§196 AGNI, approving an earlier judgment, SM before Lieven J). I think this is probably how Polly’s current care provision and condition will be interpreted.
The AGNI judgment has polarised opinion. On one hand, former Court of Protection judge Anselm Eldergill sees it as an “excellent decision” restoring liberty to disabled fellow citizens.[2] On the other hand, some charities say that it strips people of “fundamental human rights protections” in “the biggest rollback of disability rights in a generation“.[3]
This blog contributes a concrete and specific illustration of how the legal concept of ‘deprivation of liberty’ has been applied to one individual person, my sister Polly; and it explores the implications of the AGNI judgment for Polly and her family.
Part 1 introduces Polly as a unique individual with her own particular set of values, beliefs, wishes and feelings about liberty.
Part 2 outlines Polly’s deprivation of liberty following her brain injury and examines how, in practice, DoLS operated for her under Cheshire West. First, I highlight how DoLS was simply not relevant for her in ways it’s obviously relevant for some other people deprived of their liberty (Section 2.1). Second I focus on how DoLS delivered some crucial benefits (2.2). Third I show that DoLS sometimes simply failed to deliver on its potential (2.3). Finally I consider how DoLS might have actually caused her harm (2.4).
Part 3 explores what Polly’s future might hold following the AGNI judgment. I reflect, in particular, on the role of objection and ‘valid consent’.
Part 1: Introducing Polly
Polly was in a road traffic accident in 2009 which left her with multiple physical injuries along with intra-cerebral and subarachnoid haemorrhage and severe Diffuse Axonal Injury, a particularly devastating form of global brain damage involving stretching and shearing of nerve fibres in the brain.
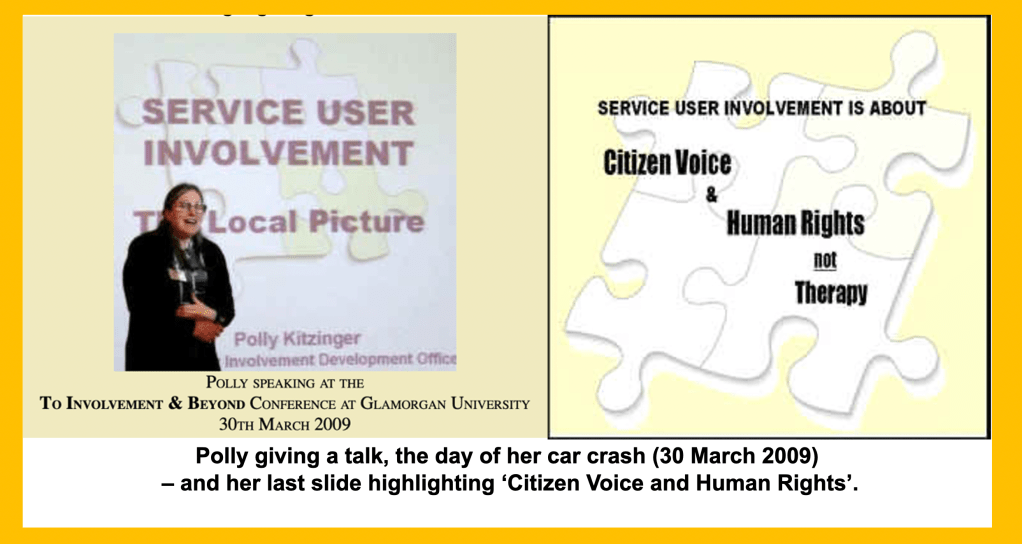
Unlike some people subject to DoLS (e.g., those with learning disabilities, whose impairments have been present since birth), people with acquired brain injuries have usually already lived part of their lives able to make what domestic law deems “capacitous” decisions. In Polly’s case, her capacitous decisions and choices were very distinctive. She prioritised freedom and adventure. Her values and beliefs were also well known by friends and family, partly because she had strong feelings about her own autonomy and also because she worked as an advocate and then a ‘service user involvement officer’ in health care settings. (For more about Polly’s work and politics, see material we’ve posted on that section of the “We Love Polly” website).
In her final job, Polly produced a leaflet about how personal stories can be used to create changes in policy and practice. It is her commitment to that, and the conversations we had as sisters about issues such as ‘privacy’ and ‘the personal is political’, which helps guide my use of her personal story now that she’s unable to author this herself, or give permission for its use.[4]
Polly giving a talk, the day of her car crash (30 March 2009) and her last slide highlighting ‘Citizen Voice and Human Rights’.
From the moment of the car crash, Polly lost the ability to make any decisions about her own medical treatment. After two years in a Prolonged Disorder of Consciousness, she eventually emerged into full consciousness with profound physical and cognitive impairments. Her presentation has fluctuated and shifted over the last seventeen years – but she’s been consistently subject to ‘best interests’ decision-making about almost every aspect of her life. For most of that time, Polly has also met the legal criteria for being ‘deprived of liberty’.
Polly was in a general hospital and then a specialist neuro-rehabilitation hospital for about a year and a half following her accident, and then moved on to a series of five different neurological rehab centres and care homes. Her care was clearly “imputable to the State” and she was “under continuous supervision and control” and “not free to leave” (the ‘acid test’ from Cheshire West in 2014).[5]
Every DoLS assessment carried out so far (these started in 2014) has found that she’s deprived of her liberty and also that she lacks capacity to consent to her residence and care arrangements because, for example, “Miss Kitzinger…presents with global cognitive impairment…disorientation to time, place and person, and lack of insight into her care needs” (DoLS form 3a, 2023). None of the extensive efforts at treatment or rehabilitation, fine-tuning pain medications, and exploration of technological aids or alternative care packages has altered this.
Polly’s physical and mental impairments severely restrict what she can do, her awareness of herself, and how she understands the world around her. She demonstrates some memory of her early life and can show flashes of compassion, intelligence and humour, but does not know that she lives in a care home (except, for brief moments, when someone informs her of this fact), and can’t remember what has happened even ten minutes ago.
She also seems to lack a sense of cause and effect: she cannot identify a source of pain or realise she needs help and then press a call bell. She is hemiplegic because her brain does not ‘recognise’ one side of her body and she’s dependent on others to hoist her out of bed, change incontinence pads, wash and dress her, spoon feed her food of the appropriate texture for her dysphasia, give medications, and transport her within, and outside of, the place where she resides.
The concept of liberty was very important to Polly, as it is to many people. It is a hugely evocative concept in politics, public discourse and in personal and family life. It’s represented by the Statue of Liberty overlooking New York harbour and personified in Delacroix’s famous painting as the bare-breasted woman leading the crowd over the barricades during the French Revolution. Liberty is symbolised by the broken chains in iconography associated with class struggle and the civil rights movement and it’s a core concept for the disability rights movement. However, as Alex Ruck Keene points out, in the law terms such as ‘deprivation of liberty’ have“autonomous meanings that do not correlate exactly with their ordinary usage”.
Polly has lived her life in the context of both the ‘ordinary usage’ of ‘liberty’ with its powerful social and political symbolism, and also the more peculiar legal definitions created by judicial interpretation of mental capacity legislation.
- 1953 (about eight years before Polly was born) Article 5 of the European Convention on Human Rights (ECHR), which guarantees the right to liberty and security, came into force.
- 1998 (Polly was in her 30s) the ECHR was incorporated into UK domestic law through the Human Rights Act 1998.
- 2005 (7th April) The Mental Capacity Act received Royal Assent.
- 2007 (1st October) The core provisions of the Mental Capacity Act [MCA] 2005 came into full force and Polly discussed this legislation with her family and prompted our mother to draft an Advance Decision to Refuse Treatment. Polly’s car crash was 18 months later (30th March 2009) when she was 48.
- 2009 (1st April) The Deprivation of Liberty Safeguards [DoLS] (an amendment to the MCA 2005) came into force. This was just two days after Polly’s accident, while she was still in intensive care.
- 2014 (March) Cheshire West – following legal proceedings based on an initial interpretation of the statutory meaning of ‘deprivation of liberty’ that played out during Polly’s early post-injury years, the definition was refined and expanded in the Supreme Court “Cheshire West” judgment in March 2014.
Polly was actively engaged with questions about ‘liberty’ (in the broadest lay sense of the term) long before she herself became subject to ‘Deprivation of Liberty’. Her views – vocally articulated before her car crash – were informed by evolving legal and political debates about liberty at the time and by our own family history and context. From childhood onwards, family conversations included: our father’s experiences in Nazi Germany and his child refugee journey to the UK; our mother’s campaigning for women’s rights in childbirth (including women in prison); and other family members’ experience of psychiatric hospitalisation and sectioning under the Mental Health Act 1983.
In adulthood, Polly’s opinions developed through her ongoing personal experiences, political activism and her professional work in diverse roles supporting people who wanted their voices to be heard, especially around health choices. This included, at one point, working for MIND as an independent advocate in a secure psychiatric unit – until she was banned from entering the premises because, in her account of this, she’d been ‘too challenging’ to the staff.
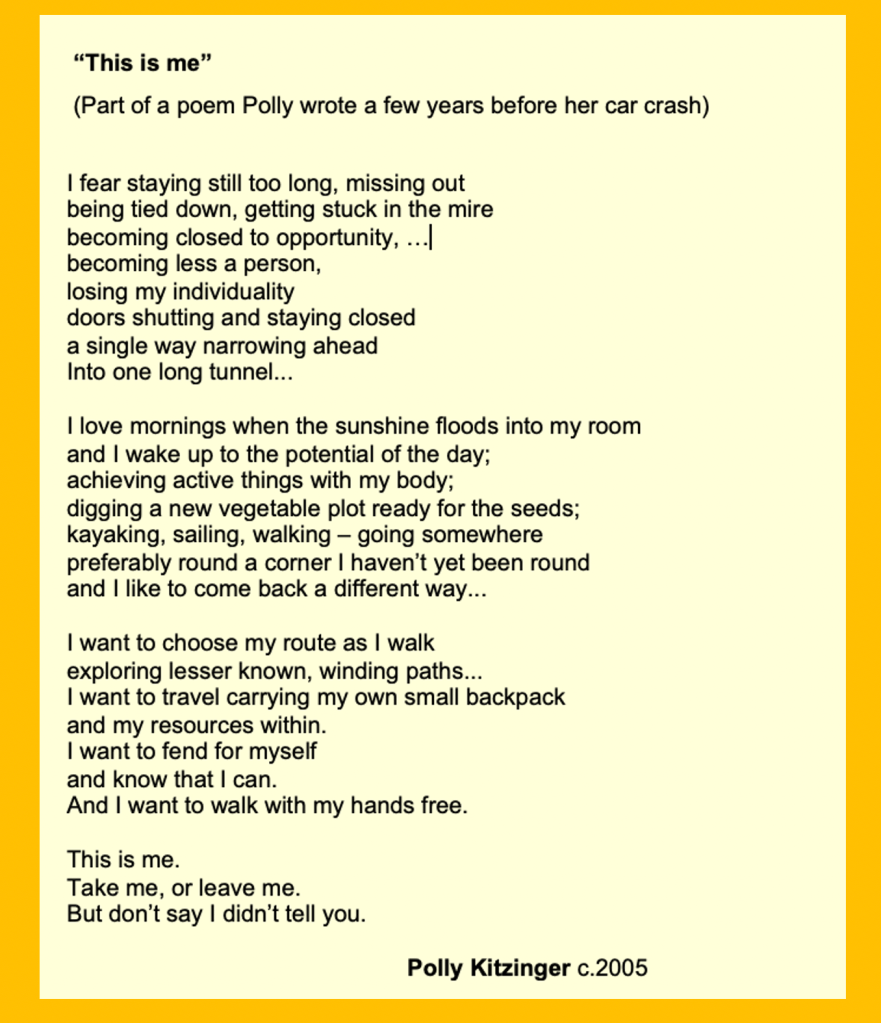
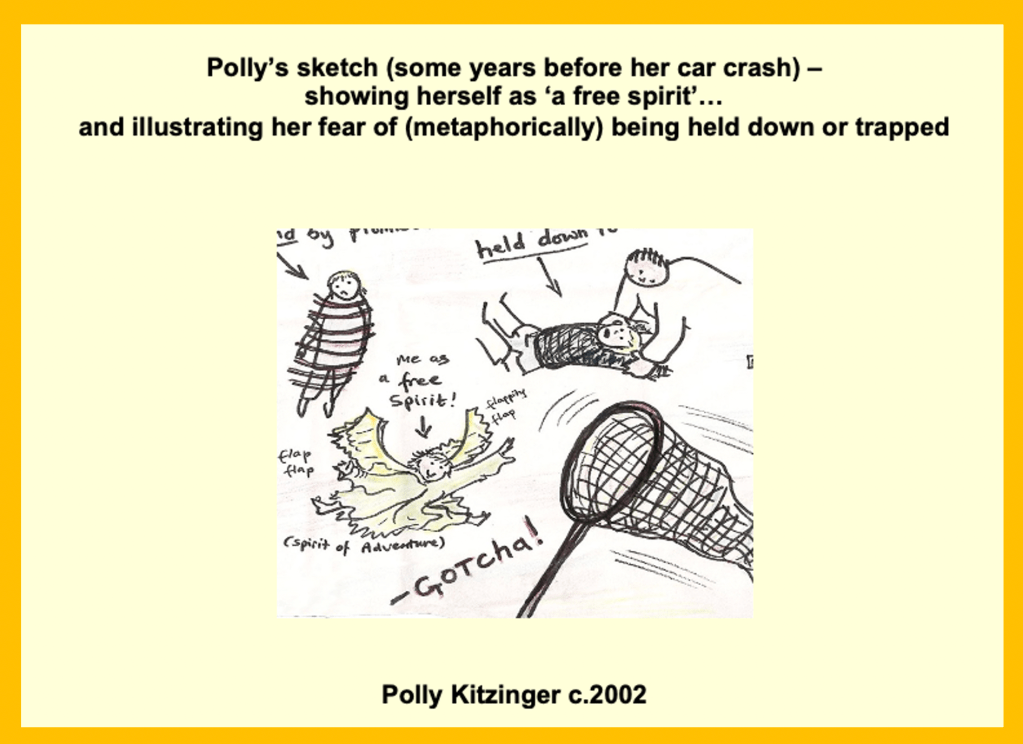
Polly was also strongly committed to her own personal autonomy. She’d refer to the fact that she’d been ‘born free’ – at home (not in hospital) in a village called ‘Freeland’; joking that this set the scene for her approach to life. She was adamant that she’d never want to live under state control, in an institution or a care home; for most her life she didn’t even want the compromises involved in sharing a home with a partner. Independence was core to her sense of self. She expressed this in the way she chose to live her life and in letters she sent us, as well as in poems and pictures.
Polly’s freedom to live her life in accordance with her own choices, value and beliefs was taken from her after her car crash. Polly’s sisters, parents and others close to her testified that Polly would not want to risk surviving with catastrophic brain injuries but doctors decided to continue to impose life-sustaining interventions upon her. Their position was supported by the ways in which the socio-medical system operated at that time. (We’ve written about this elsewhere see: “M,” Polly, and the Right to Die” and “Doctors wouldn’t let my sister die”.)
Seventeen years on, three of her sisters (Celia, Tess, and I) continue to try to fight for Polly (our parents have now both died and others close to Polly have drifted away). We keep on trying our best to mitigate the ongoing harm to her and make her life the best it can be. We take different roles.
- Celia focuses on legal developments, researches key areas about Polly’s care and liaises with lawyers. She was instrumental in lobbying for Polly’s first DoLS in 2014 after Cheshire West.
- Tess focuses on day-to-day support for Polly. She is most adept at understanding Polly now and helping her to communicate as much as possible. She became Polly’s Relevant Person’s Representative (RPR) once a DoLS was in place.
- I am Polly’s Welfare Deputy and have responsibility for the best interests decisions authorised by my court order. I make those decisions after consulting with those involved in Polly’s care or “interested in her welfare”, and taking into account Polly’s “past and present wishes and feelings” etc. as specified by s.4 MCA 2005). A Welfare Deputy must be consulted about deprivation of liberty and can veto an authorisation but cannot give valid consent to the person’s confinement. (The same applies to anyone the person had appointed in advance as their Attorney for Health and Welfare).
Part 2: What Cheshire West and DoLS meant for Polly and her family
When the Cheshire West judgment was published in 2014 it resonated powerfully with us as Polly’s family. Its principles and its symbolism seemed hugely important. It recognised the necessity of safeguards and the responsibilities of confinement “imputable to the State”. We certainly endorsed (and still do) Lady Hale’s oft-quoted statements that “A gilded cage is still a cage”. Our mother, Sheila Kitzinger, particularly liked that statement as it connected to some of her work on power dynamics in hospital maternity services (which she originally highlighted in the 1960s in her first book ‘The Experience of Childbirth’).
The ‘gilded cage’ has continued to be a powerful metaphor for us as Polly’s sisters, in ways perhaps not intended. So far, between two and three million pounds has been spent on Polly’s care by the State (i.e. taxpayers). This is, literally, around twice her weight in solid gold (at the market price at the time of writing). Even her ongoing (now reduced) core care package is £1950 per week, ie over £100,000 a year; sothis figure could increase to four million pounds given estimates of her current life expectancy. This figure would have horrified Polly who had strong views on patient-centred and just distribution of health care resources.
Expenditure does not, of course, guarantee the quality of provision, but among all the dilapidated buildings, stressed staff, under-resourced and at times chaotic health and social care system it’s also clear that Polly has sometimes had access to state-of-the art medical equipment, excellent rehabilitation facilities and some superb specialist support and day-to-day care from dedicated professionals.
The places in which she is confined have also (usually) been made to look as pleasant as possible and staff often work extremely hard to create a positive ambiance. Her first placement after leaving the general hospital was on the ward of a slightly decaying Victorian country house, adapted by the Red Cross for World War 1 ex-service men. It remained in use as a rehabilitation centre until 2020 and had a hydro-therapy pool for patients, colourful pictures on the walls, and a fish tank in the reception area.
Later she moved into modern units – designed to maximise light, air and accessibility. She currently lives in a purpose-built care home in the grounds of a former stately home. Her room has a little veranda with potted plants and the unit is as ‘normal’ and ‘home-like’ as possible. We’re pleased that Polly has a view of mature trees from her window. It’s a placement we resisted because it’s a dementia centre into which she was essentially forced when a placement needed to be found urgently, and the Health Board responsible for her NHS Continuing Healthcare package declined to fund the specialist neuro-care centre we’d have preferred – but she seems quite ‘settled’ there now. There is a simulated bar in the residents’ lounge, folded napkins on the dinner table, and regular activities such as in-house films, quizzes and live group sing-alongs.
None of this alters the fact that Polly is trapped in a life she would have refused if she’d been at liberty to do so – no amount of money can change or disguise that. ‘A gilded cage is still a cage’.
But what can (and can’t) DoLS do to help make her placements as least restrictive as possible?
The AGNI judgment prompted me to systematically review what DoLS has done for Polly in the twelve years between spring 2014 and summer 2026. I’ve organised my thoughts into four categories relating to times when DoLS has been (1) irrelevant (2) beneficial, (3) unrealised and (4) harmful.
2.1 When DoLS is irrelevant
The Deprivation of Liberty Safeguards framework is designed for a very specific purpose in relation to ‘physical liberty’ – and this is narrowly defined. The safeguards are not designed to address medical treatment as such, so trying to get a DoLS was of no use in stopping doctors from providing life-sustaining treatments contrary to what we knew would be Polly’s wishes (between 2009 and 2011). Nor did it help in challenging the associated restrictions that giving those treatments sometimes required.
By the time she did get her first DoLS (in 2014, around 5 and a half years after the car crash), Polly was no longer dependent on life-sustaining treatments such as clinically assisted nutrition and hydration so there was no obvious medical treatment we could ask doctors to withdraw. And by that time (belatedly), health care professionals concurred with family about what ceilings of treatment were in her best interests.[6]
The major residence issues that have been problematic for Polly have also often not seemed to be something DoLS can assist with. Arguments about deprivation of liberty were powerless in the context of key determinants of her placements and care such as what placements were available, what the CHC would pay for, and problems with the business models or stability of the care sector.[7]
Other situations in which DoLS is designed to help have simply not been relevant to Polly’s particular situation. There is no argument, for example, that she might have capacity to make her own decisions about residence. There’s no option to return to her own home. There are no complex discussions to be had about issues such as using the internet or going out unaccompanied (she simply can’t).
We’ve not needed scrutiny of ‘extreme’ restrictions – partly because the severity of Polly’s physical impairments means that staff can simply usually walk away from ‘challenging behaviour’ without the need for restraint. Her ability to physically self-harm is minimal and episodes of refusing food and fluid have tended to cease within 72 hours. Although we know these sorts of issues come up repeatedly in DoLS cases (especially s.21A cases) in the Court of Protection, they simply aren’t relevant for Polly. Very few cases (an estimated 1% of people with DoLS)[8] result in proceedings in the Court of Protection (some of which can bring about such vital changes for the protected party). Some lawyers are simply not very familiar with the other 99%!
2.2 When DoLS has benefits
Where DoLS has been useful is in relation to day-to-day care management issues. Ironically, this was never intended to be the purpose of DoLS (which is about the proper implementation of Article 5). However, Best Interest Assessors (BIAs) are very adept at spotting ways of improving care planning. and this has been, in practice, an important benefit to the thousands of people who have DoLS reviews, but who never make a Section 21a challenge or other court application.
The BIA is independent from both the family and the managing authority. They can bring a different focus and fresh eyes compared to those of us entangled in the morass of challenges involved in supporting a profoundly disabled person – either as a relative or as a healthcare professional. The BIA also has the authority to see all relevant documents and is recognised as an expert whose recommendations should be taken seriously – and might even recommend ‘conditions’ to the Supervisory Body which, if imposed, must be followed for the DoL to be lawful.
We’ve welcomed the fact that Polly’s BIAs can review all the documents, give close attention to Polly and her situation, and ask questions that we may not have considered. They’ve also been able to reassure staff about the use of devices such as a lap belt – underlining, for example, that staff should follow the guidance from the neuro-physio and specialist wheelchair assessor about doing up Polly’s lap belt and that this has been assessed as necessary, proportionate, and in Polly’s best interests. (The lap belt merely stops Polly sliding onto the floor; it does not prevent her moving in other ways, because she can’t.)
This never should have been an issue that DoLS needed to address of course. It should have been resolved by proper engagement with best interests, but in a unit unused to people with Polly’s type of impairment and lack of body tone, staff frequently forgot to do up the belt, and two even declined to do so when asked by me or Tess, citing ‘deprivation of liberty’ as a reason.
BIAs have also often managed to engage with Polly sensitively, listen to family concerns, and tried to maximise the ‘normality’ of Polly’s placement situation or promote her ‘access to the community’. For example, several BIA reports have stated that Polly should be included in more activities or taken out more often – and these have sometimes been set as ‘conditions’ of the Standard Authorisation.
It should not be this way of course; but our experience as family members (even when one of us is Welfare Deputy and another is RPR) is that we are often not listened to in the same way as a BIA. We can be dismissed as ‘hyper-vigilant’ or ‘serial complainers’ and we also face the complex task of trying to navigate on-going relations with care staff and organisations.
Navigating relations with staff/organisations is a particularly pertinent issue for us as we live under the shadow of Polly having been evicted from one placement after we made a series of complaints (including one about an incident of disproportionate and unnecessary use of restraint).[9] The relationships with staff became very fraught. Tess’s freedom to enter the care home was restricted – an echo of Polly’s own experience when she was banned from the premises of a psychiatric unit where she worked. Polly herself was then evicted.
Tess feels very strongly about the values of DoLS and its ability to help Polly. When I asked her about her views for this blog, she highlighted the value of being Polly’s RPR (not ‘just a sister’): “It feels like a protection for me. – that I have some validity as a visitor and someone with opinions about how my sister should be cared for. Whether that can be leveraged a tiny, tiny bit. It’s not just about whether she’s behind a locked door. It should allow me to enable her to have choices, even behind that locked door…I think DoLS is really important, it’s just another tiny corner of hope families have for making some changes.” (A longer part of this filmed interview is available at: https://www.youtube.com/watch?v=AgmtMvo2Myo).
2.3 When the potential benefits of DoLS are unrealised: A system under stress
I am less positive about DoLS than Tess. Maybe that’s because I don’t have the threat of losing the status of RPR, or maybe I have less tenacity in holding on to hope. Most of all, though, it’s because the DoLS system has often not worked as it was supposed to. The gap between the principles underpinning DoLS and the practice on the ground – and the huge unrealised potential that reflects – is crucial to considering the future of DoLS.
Our experience during the last 12 years is that DoLS has often been missing (2.3.1), ineffective (2.3.2) and/or has led to perpetuation of misleading and inaccurate information about Polly (2.3.3)
2.3.1 Missing DoLS years – unlawful deprivation of liberty
During the twelve years between 1st April 2014 (after Cheshire West) and 31st March 2026, there were, in total, almost seven years when (everyone accepted at the time) Polly should have had DoLS in place, and did not.
This surprises nobody. It’s accepted that there were simply too many cases to process after Cheshire West and that the system wasn’t equipped to deal with that volume. The result was that a large proportion of people deprived of their liberty by law, were also deprived of the safeguards that the law, in the shape of the Cheshire West judgment, had ruled should be in place to protect them. This was, as Alex Ruck Keene highlights, morale-sapping for professionals forced to prioritise who got DoLS and who didn’t; they were left effectively “having to identify how best to break the law”.
For us, as family, the message was that depriving Polly of her liberty unlawfully was not taken very seriously. It made a mockery of what had been determined by law to be Polly’s ‘rights’, reflected a gulf between law and practice, and created another fruitless task for me trying to chase up missing DoLS. The very mechanism that was supposed to “protect” her became yet another example of the broken system that now controls Polly’s life.
2.3.2 Ineffective DoLS
It’s our recurrent experience that DoLS simply doesn’t deliver on-the-ground change. For the five years when DoLS was actually in place, we were disappointed to realise that BIA recommendations and conditions often promised more than they delivered – as illustrated by the examples below
Example 1: In 2020 (maybe partly due to the start of the Covid crisis) nobody, not even the care home manager, received the relevant DoLS paperwork that should have been sent out and this was despite repeat chasing. A year later, when I was lobbying for the next DoLS, the care home manager wrote: “We never received the paperwork from the one submitted last year and we requested it several times, even during the review that was done over the phone, this was stressed out to the review officer…. I will contact them immediately to submit the new application and explain that if there was any recommendations, we couldn’t have complied with them.” When I finally did receive the paperwork I found, in fact, that it had included not just recommendations, but actual conditions (for more activities and outings). These conditions had never been communicated or monitored. Ironically, and despite the failure of the DoLS, I think in practice progress had been made on these ‘conditions’, as there was good communication and collaboration with this manager and Polly’s key worker at that point. But in terms of effective operation of DoLS, it’s obvious, at the most basic level, that the value of setting “conditions” depends on communicating with the managing authority about what those “conditions” actually are.
Example 2: A couple of years later there’d been a long gap without a DoLS. The care home manager who’d sent me the email I’ve quoted above had left (as had Polly’s key worker) and there’d been a rapid turn-over of staff accompanied by an equally rapid deterioration in Polly’s care. We’d lobbied for DoLS for a long time, and kept being fobbed off with promises that it was in the system, or that an assessor had been assigned and that it would be done soon. A BIA was finally sent in – and she carried out a thorough consultation and review resulting in a detailed and extensive set of conditions. Those might have been helpful had they been imposed earlier – but, in fact, the care home closed down a few weeks later after severe staffing problems and being rated Inadequate by the CQC.
Example 3: Even when DoLS recommendations or conditions are in place and known about in a timely manner, it has taken huge efforts to deploy them in the service of even a tiny improvement in Polly’s life. It needs concerted efforts, week after week, to make progress that is often only temporary. For example, a “condition” stating that Polly should have the opportunity to be taken out of the care home at least once a week may be thwarted by, for example: first finding that her large wheelchair can’t be safely accommodated in the care home van along with other residents that are to be taken out that day; next, when they finally get her into the van, finding the necessary securing tension strap is broken; the third week there is no outing at all because the driver is off sick, and there is no cover. Other reasons outings didn’t happen have been that the van is needed for another resident’s hospital appointment, Polly herself has an unannounced visit from the dentist and we decide that should take priority, or Polly is too exhausted or agitated at the scheduled day and time. When it finally does happen, the “outing” may constitute nothing more than being put in a van and driven around a lake without even being taken out of the vehicle. But Polly has “had an outing” and the box for that week is ticked, on paper at least.[10]
Example 4: There is considerable variability in the skills and practice of BIAs (or perhaps challenges they face with conditions of employment and pay). This can mean the whole DoLS process is at best a lost opportunity. The BIA who assessed Polly in 2025 did not contact us in advance of going to see her. This meant that neither Polly, nor he, could benefit from what we might have told him in advance, nor could we offer to provide Polly with communication support. He only rang Tess (Polly’s RPR) and me (Polly’s Welfare Deputy) the week after seeing her – and then informed us he urgently needed to submit the report by the end of that day. My initial conversation with felt too brief (I was travelling at the time): he did not get back in touch when I asked him to, nor did he discuss his report with us in advance of submitting it, as some BIAs have done in the past. His report included significant errors of fact.
2.3.3 DoLS paperwork can perpetuate misleading information and errors of fact
I have become accustomed to sometimes ignoring and sometimes playing ‘whac-a-mole’ with the misinformation that frequently results from the copy-and-paste process of paperwork about Polly. Inevitably, BIAs are having to edit and process unfamiliar information at speed and the relevant forms often seem to involve the need for multiple repetition of similar information in different ways, without those completing the forms always having access to the relevant authoritative source. This means out-of-date information lingers and other information morphs and changes to the extent that it sometimes ceases to bear much relation to reality. The format of the forms themselves seem to breed data degeneration.
Even when reviewing the DoLS documents produced by the professionals I think were good there are errors. For example: one report says that the BIA consulted Polly’s sisters and her children (she doesn’t have any children). Another DoLS document says that Polly kicks out at staff with both legs (she can’t – she’s paralysed down one side). A third states that Polly is being taken on visits to her family home – but this was claimed long after our father had died and the family home had been sold
Some of the reports include what might pass as detailed legal analysis if we didn’t suspect it was simply cut and pasted from another source. In assessing Polly’s understanding of the salient points about her care and the impact of her brain injury on her decision-making, one assessor cites Derbyshire CC v AC, EC & LC [2014] EWCOP 38 and PC and NC v City of York 2013 and refers to the “Causative Nexus” (Form 3a, 2023a). Another assessor claims to use ‘the Guzzardi framework’ to analyse the restriction on Polly (Form 3a, 2025). It’s superficially impressive – but it feels as if Polly herself has become lost in the process. In some reports the tell-tale signs of copy and paste are sometimes betrayed by pronoun changes (e.g. Polly is referred to as ‘he and ‘him’ mid-sentence) or odd shifts from “Miss” or ‘Ms’ to ‘Mrs’ (she was never married and would have vehemently objected on feminist grounds to both “Miss” and “Mrs”).
Forms also include slightly bizarre statements such as “Miss Kitzinger has no awareness of what is a healthy balanced diet” or “If she left by herself she would become lost” (Form 3, 2017). These are bizarre (to us) because planning a balanced diet or finding her way around are so remote from Polly’s actual capacities as to sound fanciful. Apart from propelling herself from bed to crash mat when thrashing during periods of agitation, Polly can’t independently mobilise at all.
Errors and irrelevances sometimes result from what we have come to think of as ‘performative personalisation’. By this we mean that professionals attempt to display familiarity with the individual, and to demonstrate that they’re considering Polly’s best interests ‘as a person’. Of course, acknowledging who the person is/was can be done skilfully and well – and we appreciated the BIAs who took the time to listen and acknowledge something meaningful about Polly. But some assessors’ representations of who Polly is/was can be very shallow and unconvincing.
The 2025 DoLS paperwork is a prime example. The BIA reproduces incorrect information from earlier forms and adds some additional factoids of his own.
- Form 3 asserts that Polly was born in Oxford: she was not – and the fact that she was born in Freeland was, as I’ve highlighted earlier, very important to her. It says that she also went to school in Oxford. She did not. It reports that:“At school, she enjoyed drawing and writing poems. She did not like Maths” (Form 3, 2025). Unlike the first two ‘pseudo-facts”, this last point is true, but seems a strange thing to highlight. We haven’t been able to trace where the BIA obtained the ‘dislike of Maths’ factoid: it’s certainly not information we would ever have raised as relevant to DoLS, but was perhaps something one of us mentioned in passing to a carer or activity co-ordinator. It seems very odd to put this on a DoLS form, over 40 years after she left school.
- More seriously, under the heading ‘Past View” the BIA went on to state (manifestly falsely) that: “There is no information on record of an advance decision or past views/wishes expressed by Ms Kitzinger in relation to care/accommodation”.I don’t suppose anyone reading this blog post will be surprised to learn that I’ve placed a one-page summary about Polly’s “past views/wishes” with her hospital admission pack, alongside my detailed and evidenced Welfare Deputy report. There are also, of course, the public statements we’ve made about Polly’s past values, feelings, wishes and beliefs, including an interview with BBC news.
- The final paperwork from the Supervisory Body states categorically: “The Supervisory is satisfied that the Best Interests Assessor is assured that there is…no Deputy for Health and Welfare”. Who can have “assured” this BIA that there is no Deputy for Health and Welfare? Certainly not me, her Deputy for Health and Welfare. How can the Supervisory Body be “satisfied” that the BIA is so “assured”? The fact that this form was signed off and filed to “protect” Polly and “safeguard” her is ironic. It was probably “just” cut and paste – but it’s an egregious error.
In the 2025 DoLS documentation, Polly’s identity as an adult and the extensive evidence of her strong values and beliefs (her sisters’ ability to represent these and my particular role in promoting her best interests) is simply erased. The documentation leaves a gap between Polly as a schoolgirl who didn’t like Maths and Polly as the care home resident she is today – the Polly we knew for her entire capacitous adult life is rendered invisible.
2.4 DOLS Harms
All interventions (whether administrative or medical) can carry both benefits and harms – the point is to be aware of the potential for both, and to maximise the benefits and minimise the harms.
Mostly I’ve felt that DoLS has not harmed Polly directly, but reviewing relevant documentation for this blog has led me to revise this opinion a little.
The spectre of DoLS, and (erroneous) views about it by front line health care staff, may sometimes have interfered with thoughtful best interests decisions and care for Polly. For example, in October 2014 (just after we’d successfully initiated the first DoLS process) we discovered that Polly been left in bed for over a week. This was contrary to her care plan and therapists’ advice, especially in relation to managing her chronic pain at that point. There was no evidence that any significant time had been spent reassuring Polly ahead of the necessary hoisting or even give her a reason for getting out of bed (such as an opportunity to be taken out of the care home).The manager’s response to our complaint was that this decision accorded with Polly’s own wishes not to transfer to her wheelchair. She wrote: “There is no Deprivation of Liberty safeguard in place for Polly and as such we need to remain responsive to her wishes as she indicates them“. The letter concluded with the result of the investigation of our complaint: “Outcome – Unsubstantiated” (Letter from manager, 22nd October 2014). This illustrates the anxiety staff may have about attempting to persist with some interventions when a person says no. It also reveals a confusion between DoLS and Best interests.[11]
The second potential harm to Polly relates to the assessments themselves. It’s well-documented that some care home residents experience the BIA process as intrusive or distressing (see, for example, “A court hearing and 23 visits from 16 officials”). I do not think Polly has usually experienced them this way – not least because Tess has usually been there to mitigate any distress that might result from the questioning and to ensure that Polly is understood as much as possible (Polly’s speech is very limited and difficult to understand). However, looking closely at the report from the BIA assessor in 2025, I think this assessment may have caused distress. This was the year we received no prior notice of the assessor’s visit to Polly: he met her with a ‘senior carer’ but no family member. He describes arriving to find Polly relaxed, calm, and alert, but his account suggests to me that she quickly became disengaged. Here’s his record of the interaction:
Best Interest Assessor Form 3a, 2025 – ‘Functional assessment’ section
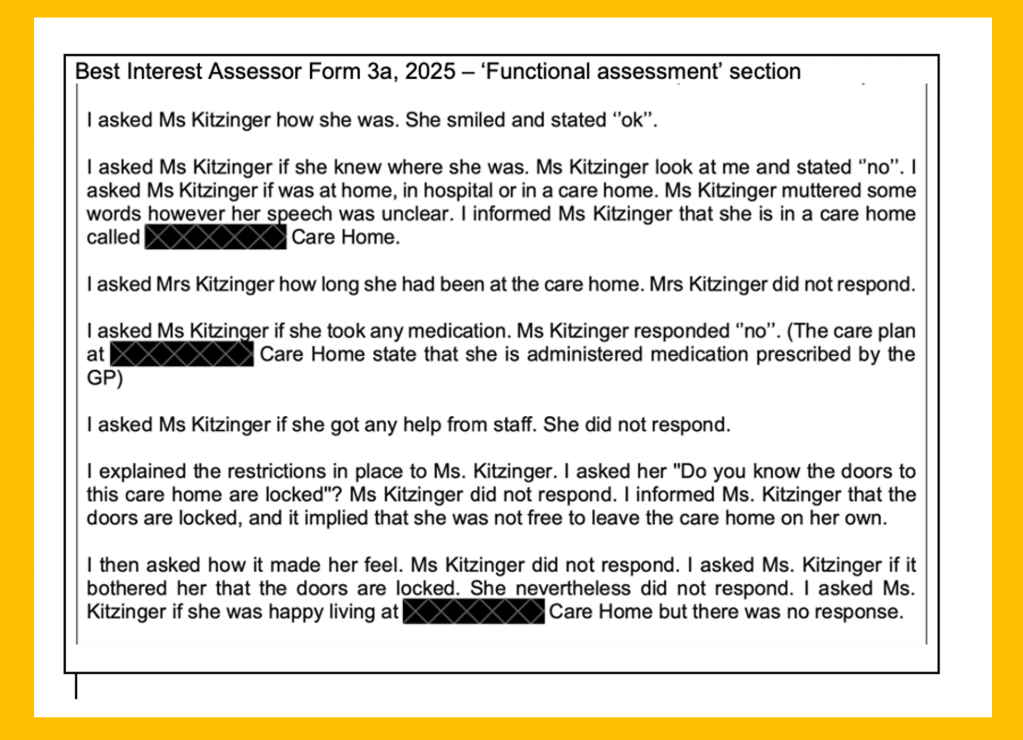
I do not think this was handled well. We know from our own interactions with Polly that when told she’s in a care home, she can respond with shock and repeatedly ask ‘Why? Why? Why?”. She can also become distressed when quizzed about a reality she does not recognise (e.g. that she needs support and is living in a locked environment). I suspect Polly forgot this encounter within minutes – and I hope any distress it caused faded quickly too. But I’m going to request that in future no formal assessment on Polly is done without informing me or her RPR in advance and ensuring that Polly has the option of having one of us present for the assessment.
3. Looking to the future: objection and consent
I assume there will be at least one last DoLS assessment of Polly to check whether or not she remains eligible for DoLS. The multi-factorial approach will necessitate some consideration of objection, and I suppose it’s possible it might also (depending on the flow chart followed) consider the concept of ‘valid consent’. In this last section, then, I want to reflect on how Polly’s behaviours and views in these domains were interpreted prior to the AGNI judgment, and how this might be different post-AGNI.
On objection: For almost ten years after Polly regained consciousness she could display very “challenging behaviour” and what the nursing assessments record as “violence against herself and others”. This necessitated funding for one-to-one support at times and specific management strategies. Sometimes the ‘triggers’ could be clearly linked to specific actions (such as giving personal care), her chronic pain, or sources of obvious frustration (such as no one being able to understand what she was trying to say).
But sometimes no specific ‘trigger’ could be identified (in spite of all the ABC charts and monitoring) and at times there were intense periods of shouting and kicking and refusing care and treatment, as well as food and water. The most intense episodes could be accompanied by increased lucidity and ability to communicate. They seemed linked to internal distress; she could occasionally shout or write legible words during these episodes – sometimes recording emotions and desires including, on one occasion, quite remarkably, writing: ‘I‘m thinking how to die’, ‘kill me’, “I need to kill myself”. A psychiatric assessment was carried out in 2012 using an ‘Ill-being’ scale’: it gave Polly the highest possible ratings on all dimensions including: “shows signs of feeling depressed or despairing”, “shows intensely angry or aggressive behaviour”, and “shows signs of grieving over losses”.
Polly’s “challenging behaviour” or expressions of distress have never been interpreted as Polly objecting to her placement. Nor has documentation of her prior wishes (never wanting to live in an institution or care home) ever been used to inform such a conclusion. She no longer displays such behaviour – but were these episodes to recur, I think it looks like ‘objection’ might get more attention in the post-AGNI legal, policy and practice landscape (e.g., see AGNI para 145).
On ‘consent’: Ironically it is ‘valid consent’ which now, at least in theory, might be more relevant to Polly (if the objective measure for ‘deprivation of liberty’ were to be met, which I don’t think it will be). Polly’s behaviour has changed dramatically in recent years. She is now super-compliant and seems eager to please. She may still briefly become agitated by things such as if another resident who is mobile walks into her room and touches her – but otherwise Polly seems not to complain about anything; in fact she seems no longer to attempt to communicate her experience at all. Her care notes record her as “settled” and “cheerful”.
A recent psychiatrist’s report prepared for the last DoLS writes that Polly is “very compliant” and is “happy with her care” (Form 4, 2025). She often smiles a welcome to people who come into her room and starts shouting “I love you” repeatedly over and over again (to care staff, GP, dentist, and to the best interests and mental capacity assessors). When, a few weeks ago, Tess tried to explain to Polly that she was living in a care home and ask her about her experience of it Polly replied “I love you”, then “you’re lovely’. When Tess again prompted Polly to talk about the care home she responded “it’s lovely”.
I would like to think some of the changes in Polly’s might be linked to changes in her actual experience. I don’t think she’s got the memory or processing power to ‘adjust’, ‘come to terms’ or discover new meaning in a radically changed life (a common journey eloquently reported by people facing sudden-onset physical disabilities such as spinal cord injury). But perhaps her brain has changed in ways that mean she’s less tormented by flashes of memory or insight that seemed to me to be associated with the earlier most intense and sustained outbursts of rage and distress. I wonder if she’s now developing post-brain-injury dementia and losing a deeper layer of memory in some way. Or perhaps her care and the nature of her placement has changed in ways which keep her calmer?
But I also see the force of the explanation advanced by my sister Tess, who is closest to Polly – and her perspective is much more disturbing. She believes the changes in Polly’s behaviour were, in part, linked to the Covid restrictions, when we were often unable to visit her. The effects of the pandemic lockdowns were exacerbated for Polly as staffing and management of her care home deteriorated. Its CQC rating dropped from “Outstanding” to “Inadequate” – with failures in safety, caring, effectiveness, responsiveness and leadership. The CQC report records that “Staff members did not always treat people with warmth, dignity and respect” and “People were not always supported to have maximum choice and control of their lives and staff did not always support them in the least restrictive way possible”. Tess says that Polly simply “gave up on fighting her corner”. She has been finally “broken-in”, her emotions “flattened”, she’s no longer expresses some of her needs: “It’s almost like there was no other way for her to exist but to become compliant and lock the frustration away and hide the key”.
This remains true even in the new placement she moved to – with kind staff, who are clearly fond of her, and committed to respecting her choices where ever possible and supporting her the best they can. This ‘new Polly’ will now assent to almost anything. After noticing her front teeth looked loose and askew, for example, I discovered that carers had taken a dental bridge that had broken off – and repeatedly reinserting it into her mouth (apparently under the mistaken belief it was a form of denture). She’d passively accepted, without protest, the reinsertion of the metal spike into her jaw, and the consequent lopsided bulge in her mouth as it worked loose again. On another occasion Tess tasted a spoonful of the food she’d been given to feed Polly with, only to find it had a yoghurt topping containing bitter medications – which should have been given separately and overtly by a nurse. Polly had been accepting the food and indicating that it tasted good – though it can’t possibly have done! Tess says: “She is very vulnerable in every way. She’s vulnerable to people deceiving themselves into thinking everything’s okay when it’s not. I wish she could protest more… This is a big problem because she doesn’t complain. They think they’re doing really well and they don’t understand why I have issues with some of the care“.
Although I have been somewhat reassured by the sophisticated understanding shown by BIAs when discussing how people might present, and a clear reluctance to take ‘consent’ at face value, I do share the widely expressed concerns that ‘valid consent’ is open to misinterpretation and may result in making vulnerable people more vulnerable.
4. Conclusion
Polly’s life for the last 17 years has been radically different from how she lived her life when she was free to make her own choices. She has irrevocably lost her ‘liberty’ – in the sense in which she interpreted and valued it. She would have defined herself in this situation as someone with ‘no liberty left to lose’ as she understood the concept.
We are left trying to ensure ‘person-centered’ care for her in the situation she is now in, navigating ‘best interests’ decision-making and attempting to minimise restrictions, maximise opportunities, and support what few choices she can still make.
The framework put in place by the Deprivation of Liberty Safeguards has enormous symbolic (and some real) power – and that framework has been one of the few mechanisms for regular independent review, on which we have rested our hope for improvements in her care. We have valued the intervention of skilled and knowledgeable Best Interests Assessors. But the system has also been frustrating, not always fit for purpose, and can cause harm.
Despite all this, we are deeply worried by the likely removal of safeguards from Polly. We can only hope that whatever other supports and safeguards are introduced to replace or supplement DoLS will offer something better for Polly and others like her – especially in relation to her Article 8 rights. Perhaps our family experience, as described here, can contribute in some small way to those future developments.
Jenny Kitzinger is co-director of the Coma & Disorders of Consciousness Research Centre and Emeritus Professor at Cardiff University. She has developed an online training course on law and ethics around PDoC and is on BlueSky as @JennyKitzinger
[1] “A Reference by the Attorney General for Northern Ireland of a devolution issue under paragraph 34 of Schedule 10 to the Northern Ireland Act 1998” [The AGNI judgment] https://www.supremecourt.uk/cases/uksc-2025-0042
[2] LinkedIn Post (June 2026) https://www.linkedin.com/posts/anselm-eldergill-
[3] Press release from the National Autistic Society Mencap, Mind and the National Autistic Society https://www.mencap.org.uk/press-release/biggest-rollback-disability-rights-generation-charities-respond-supreme-court-ruling; https://www.autism.org.uk/what-we-do/news/charities-response-to-supreme-court-ruling
[4] For further discussion of Polly’s views on privacy and some of my consultation about this with those who knew her, see: section 2.2 of ‘Successful application to disapply Section 12(1) of the Administration of Justice Act: Making Polly’s statutory will application public’ See also ‘Applying for a statutory will: Observation and personal experience’
[5] P v Cheshire West & Chester Council & another; (2) P & Q v Surrey County Council
[6] Lindsey Briggs brought an application under s.21A MCA 2005 challenging the DoLS authorisation in place at the hospital where her husband was being treated (and being given life-sustaining treatment in a minimally conscious state). She did so on the express basis that a s.21A application would allow her to claim legal aid on a non-means-tested basis – thus supporting legal representation to be able to argue her case that continuation of CANH was not in her husband’s best interests. The Court of Appeal in Director of Legal Aid Casework and others v Briggs [2017] EWCA Civ 1169 found that the Mr Justice Charles (in the original COP judgment on this point) had been in error in finding Mrs Briggs’ application under MCA 2005, s.21A, appropriate in these circumstances. Lady Justice King commented that: ‘section 21A goes to a consideration of whether the detention or deprivation of liberty is itself in P’s best interests and, while the surrounding circumstances are part of the picture, the question is not whether the circumstances, including the medical treatment P requires, (which amount to a deprivation of liberty), are in the best interests of P, but whether it is in the best interests of P to be a detained person.’ https://www.anthonycollins.com/insights/ebriefings/withdrawal-of-life-sustaining-treatment-and-mental-capacity-director-of-legal-aid-casework-and-others-v-briggs/
[7] I’m grateful to Lucy Series for drawing my attention to proposals by the Law Commission 2017 (paragraphs 9.27 – 9.28) to remove the ‘best interests’ criteria for authorising a deprivation of liberty. This was on the grounds that, in practice, authorisations often have to be made that are not in the person’s best interests but are the only available option. The notion of “best interests” adds nothing to the requirement that the DoL should be “necessary” and “proportionate”. (See also the judgment by Cobb J in North Yorkshire CC v MAG).
[8] Lucy Series writes: “There are no statistics on rates of appeals under the DoLS, but a best estimate puts the rate of appeal at fewer than 1% of people subject to a DoLS authorisation during 2017, and under 0.5% of DoLS applications overall” (Dr Lucy Series, Cardiff University, Evidence to JCHR on MCA DoLS, March 2018 (https://committees.parliament.uk/writtenevidence/87756/html/#_ftnref6.)
[9] Tess’s written complaint to the home manager recorded that she’d entered Polly’s room to see a carer holding down Polly’s right hand (the only one she can use) and the nurse spooning liquid medications into Polly’s mouth: “Polly was fighting it. When Polly began to choke, [the named nurse] said: ‘you see what happens when you make a fuss’ and spooned more medicine into Polly“. Tess’s formal complaint highlighted that Polly’s Speech and Language Therapist had advised that “Polly is not supposed to be given any liquid before it is thickened to a ‘whipped cream’ consistency” and “If a patient begins to choke I understand that a carer is supposed to wait at least 5 minutes or until their voice sounds clear and non watery before putting more in their mouth. [named nurse] failed to do this“. Tess also pointed out that the nurse’s comment to Polly (“see what happens when you make a fuss“) was “inappropriate especially given Polly’s level of distress and her communication and cognitive impairments“. We never witnessed such behaviour again but the fact the nurse (supported by the carer) did this as Tess entered the room, left us concerned about what might have happened leading up to this incident, and what staff might do and say to Polly when family were not present. On another occasion when I witnessed restraint that might have been disproportionate (involving staff in a different placement), I took out my phone and asked Polly if she’d like me to film what was happening – Polly nodded. As I started filming the two staff members immediately let go of Polly and stepped away, one saying in alarm, “It will look like restraint” – a comment that I thought was revealing in itself. It underlines the importance of outside scrutiny and ‘bearing witness’.
[10] There’s a huge gulf between the expectations Polly’s care homes set for outings and our own aspirations – some of which we’ve managed to achieve as a family, albeit with a great deal of time, repeated effort and flexibility. In Autumn 2010, before I understood how narrowly ‘outings’ and ‘access to the community’ are often interpreted, I produced a list of suggested trips out for Polly’s new placement based on things we’d already tried. This list now seems rather laughable. It included: “Craft fairs (especially if Polly is able to handle the objects)”; “Music events (she has tolerated short sessions …although be aware she may interrupt with sudden shouting)”; “Art Galleries (Polly was a keen artist – and one trip to an art gallery seemed particularly to engross Polly, although subsequent such visits have generated less interest)” and “Festivals (her sisters took Polly to the gay and lesbian Mardi Gras – and Polly was fascinated by the drag queens)“. (‘Service User’s Perspective: transfer summary for Polly Kitzinger’, Jenny Kitzinger, Welfare Deputy Report No 3. October 12th, 2010).
[11] I wonder if staffing shortages may also have come into play as 3 staff members were required to hoist Polly safely at this point and it took a long time to do it gently and appropriately. Working with family to support the transfer or having us there to suggest an outing with her sisters might also have been helpful, but there was little collaboration with us at this point. A formal eviction letter arrived for Polly the following month.
Endnote by Daniel Clark
Back in 2014, In Cheshire West, the Supreme Court considered the meaning of a deprivation of liberty (DoL) through reference to Article 5 of the European Convention on Human Rights. Lady Hale, giving the majority but not unanimous judgment of the Court, presented an ‘acid test’ for deprivation of liberty: is a person under continuous supervision and control, and not free to leave?
On Tuesday 2 June 2026, the Supreme Court handed down judgment in what is increasingly being referred to as “AGNI’ (the case was brought by the Attorney General of Northern Ireland). The Supreme Court overturned Cheshire West, finding the acid test to be wrong in law, and directed a different approach.
First, the identification of the objective element of a deprivation of liberty must entail a multifactorial analysis, which includes consideration of the intensity and purpose of confinement. If these conditions are not satisfied, there is no deprivation of liberty.
Second, a person may lack capacity to make decisions about their care and residence but can nevertheless give valid consent through an expression of their (positive) wishes and feelings. If a person is giving such consent, they are not deprived of their liberty.
To access the judgment, see: Judgment (PDF) (hyperlinked)
To access the court’s approved press summary, see: Press Summary (PDF) (hyperlinked)
To access the commentary published by the Open Justice Court of Protection Project, see: Commentary on the UK Supreme Court case about deprivation of liberty (hyperlinked)
If you would like to contribute a commentary about this judgment, please contact [email protected], and mark your email for the attention of Daniel Clark.

Don't Miss:
-
From Cheshire West to AGNI: Rebalancing Protection, Autonomy and Human Rights
-
Considering ‘deprivation of liberty’ in a family home setting after AGNI
-
Judge authorises medical treatment and DOLS in hospital
-
AGNI: A common-sense judgment or agony?
-
Declaration of death or serious medical treatment withdrawal?